Dion Nowoweiski: "We tailor the treatment protocol to the individual"
This is an interview with the Australian ISTDP therapist and researcher Dion Nowoweiski. We reported on one of his recent publications a while back, showing promising effectiveness of ISTDP in the treatment of eating disorders. In the interview we discuss the publication and what makes ISTDP unique in the treatment of eating disorders.
Earlier this year you published one of the first empirical articles on ISTDP in the treatment of eating disorders. How do you feel about the publication?
We’re very pleased. It took longer than anticipated but it was a real team effort from all of the authors. Each author contributed in a unique way, but it goes without saying that this publication was only possible because of the dataset that Allan Abbass has been accruing over the years.
We were able to find a small sample of patients with eating disorders who had been treated through his service in Halifax. Typically, you would find these kinds of patients presenting to specialist eating disorders services or other non-tertiary mental health services. I think one of the more interesting aspects of this study is that ISTDP may be a suitable alternative to the established eating disorder treatments currently offered, many of which show a less than 50% response rate.

In my opinion, that’s what makes this study so important. It offers an alternative treatment paradigm for the sub-specialty of eating disorders as many of the traditional treatment paradigms are limited by issues such as poor response, high dropout rates, burnout of professionals, high demand and low capacity of mental health services and high costs associated with inpatient care, amongst some of them.
Can you tell us about the background of the study?
The study was the brainchild of Allan Abbass. We had already done some work on a previous publication on eating disorders, so he approached me to ask if I would be interested in writing up an article of the datafile he has been collecting. We were trying to see if there was a case for whether ISTDP could be a valid treatment protocol for people with eating disorders and whether there was any evidence as to whether there were any cost savings for cases treated with ISTDP. This study is part of a series of publications that he's been working on in relation to showing cost savings related to ISTDP in other areas, for example, emergency departments.
Why is ISTDP the treatment of choice for eating disorders?
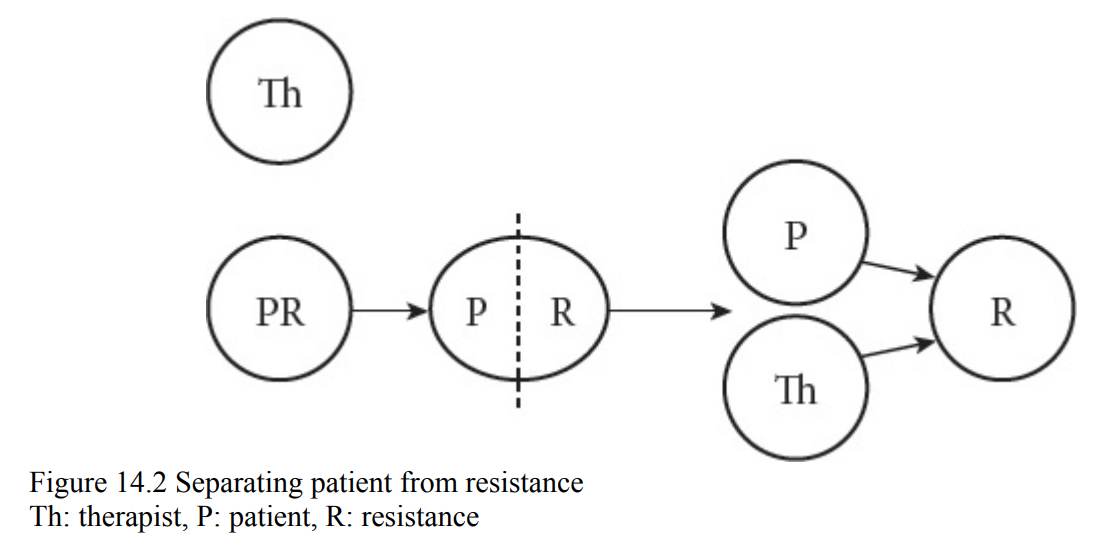
I wouldn’t say that ISTDP is the treatment of choice for eating disorders per se. But I do think it’s a very good treatment option for people who suffer from ego-syntonic symptoms. As many of you will know, an eating disorder can be a very difficult condition to treat. I believe that one of the factors that contributes to this is the syntonicity of the symptoms. Through my clinical work, I have found that a large proportion of people with eating disorders tend to value their eating disorder symptoms. They don't see themselves as separate from their resistance.
For example, for many people suffering from Anorexia Nervosa, there is a strong sense of accomplishment associated with the level of self-denial required to maintain a restrictive intake of food or with the level of self-discipline needed to maintain an excessive exercise regime. Both of these symptoms (restriction and excessive exercising) are criteria for an eating disorder diagnosis.
Yet, imposing conditions on these behaviours – which is common in many treatment models for eating disorders – fails. It’s quite possible that this fails, because the patient values these symptoms as part of a mechanism that helps them maintain a sense of self-control and reduces their fear of harm (either from being overweight or from their own impulses).
In ISTDP for eating disorders, we aren’t trying to take anything away from the patient. We’re trying to help give them choices over their life by identifying the origin of their difficulties and seeing how their eating disorder symptoms function as a mechanism that, while once might have been necessary, is no longer helpful and preventing health. By doing this, it becomes more of a conscious choice for the patient to give up the life of suffering that they had once valued. I see this as a very unique contribution of ISTDP to eating disorders.
Compared to other models that try to encourage abstinence or control over impulses to binge and purge, I find ISTDP a very helpful model as I believe it is more focused on helping people change from the inside rather than forcing someone to change from the outside.
Can you talk us through the specific things to take into consideration when initiating ISTDP for a person struggling with eating disorders?
Identifying the problem that the patient wants to work on is one of the first steps in the psychotherapy process. When you ask the standard Trial Therapy question of "what problems can I help you with?", many of them respond by saying "I have an eating disorder". Obviously, this doesn’t tell us anything about their problem.
“How is your eating disorder a problem for you?” is a usual follow up. But that depends on what else is happening when the patient answers my question: non-verbal signals and so on. Without going into those details here, the point I’m wanting to emphasize is that it’s a mistake to believe that the eating disorder is the problem. That's just a set of symptoms given a label.
But this kind of answer illustrates one type of difficulty often encountered in treating this population. It may seem like the person is saying they see their eating disorder as a problem, but on further examination we find that the eating disorder is a coping mechanism. For some people, that can be clarified early on in the Trial Therapy session. For others, I may not even get to do clarification work as their anxiety tolerance may be more problematic indicating their motivation to change is not the issue we need to address at this early stage. These cases require capacity building prior to any defense work.
The mistake I used to make was to assume that if a patient could formulate a response to my question, that meant they weren’t “over threshold”. But I’ve found that for many people with a significant and chronic eating disorder history, they have adapted to starvation and have learned to function as though they weren’t over threshold – even though they sometimes are. It’s taken time to recognize this, as it’s a different type of presentation of a person who is over threshold in the more usual ways.
Understanding the starvation effects on the brain is vital at this stage and being able to recognize whether the person sitting in front of you can think clearly is so important. They may not look like they’re over threshold or suffering from starvation affects as they can reason, but when that reasoning starts to take on a circularity to it, it’s best to evaluate whether the person is fragile. For example, when you begin to challenge circular reasoning in the form of the patient saying things like “I know I’m underweight”, but if I eat more I will get fat and then I won’t be healthy”, the patient can lose concentration, become confused, appear distant or shut down in some other way. I have learned that this usually signals issue with starvation on the brain and/or poor anxiety tolerance. It’s like saying "if you interrupt my circular reasoning (defense) and I have no other mechanism for dealing with the feelings you just triggered in me by pointing out my flawed logic, I need to protect you from the impulses attached to those feelings by dissociating."
In your recent article you mention that perhaps other treatments aren't effective for eating disorders because of insufficient attention to "structural deficits". Can you explain what you mean? Is this an ISTDP-specific thing, or would mainstream psychoanalysis suffice?
I don’t know whether this comes from ISTDP specifically or if it’s from mainstream psychoanalysis, as I haven’t read much on psychoanalysis. I’m pretty much just an ISTDP practitioner and haven’t branched out very much. I think this helps me as I suspect that trying to blend or combine models would confuse me too much and would result in me exceeding my learning threshold.
What is meant by that statement though ("structural deficits...") is that as a diagnostic group, people with eating disorders can vary so much. Not understanding the psychological capacity of the individual sitting in front of you is probably not good enough. Some cases may have a neurotic structure as described by Davanloo in that they are a resistant case with little need to restructure defenses or build capacity.
Other cases may have suffered from overwhelming attachment disruptions at an earlier age and therefore they haven't developed the same level of ego capacity as other cases. For these cases, under some level of activation of the somatic pathway of emotions, they run into problems if they only have access to the less mature defense mechanisms of projection, splitting and projective identification. Trying to offer these cases the same treatment as those with a more intact psychological structure seems unfair to me. It’s like asking someone with one leg to race against Usain Bolt and get upset with them if they lose.
I prefer a model where we tailor the treatment protocol to the individual rather than making the individual fit the treatment protocol. Unfortunately I’ve worked in specialist eating disorder services where the latter is the common service model and it used to frustrate me to see how patient’s would be selected for treatment based on whether they met the requirements of a specific treatment modality based purely on the history of the person, without even considering the psychological makeup of the person.
What are some of the main challenges doing ISTDP for ED?
Many of the challenges I’ve encountered when working with people suffering from an eating disorder from an ISTDP perspective can be categorised as 1) relating to the individual and 2) relating to the broader treatment system.
The issues relating to the individual are linked to what I mention earlier and is about working with a syntonic defensive system and working with fragile clients where capacity building is needed. As you know, and as explained by Allan, in ISTDP we need to complete a thorough psychodiagnostics assessment. This begins at the outset of treatment and is focused on helping us identify the structure/organisation of the defensive system we’re working with and the degree to which the defenses are syntonic to the patient. We also need to know about the anxiety discharge pathways and whether there is a threshold to smooth muscle activation or cognitive-perceptual disruption. And at what level of rise in the complex transference feelings the different thresholds are crossed.
Although these may sound like simple enough concepts on paper, the ability to recognize what this looks like in the room, when we’re working with a patient, is something that needed to develop over time and came with doing more treatment for me. As I’ve did more and more treatment, my ability to be confident with my skills improved as I felt more comfortable with my assessment of what’s going on in the patient. This was something that I found needed to be done more collaboratively with patients than what I had been doing early on in my career. In the beginning of my career, this was something that I didn't understood properly. But over time I found that the more I collaborated with the patient on what I was observing, the more feedback I got and the more conscious alliance it created.
The other issues relates to doing ISTDP work in a field that appears to be quite static (as opposed to dynamic). The mainstream models of treatment for eating disorders are sometimes quite narrow and I found them somewhat punitive at times. During my time working on inpatient services, I found that the model was very rigid and my efforts to step outside of that framework were usually met with quite a bit of resistance from others. What I learned from this has been invaluable for me, because it really taught me that we operate – as therapists – within systems and these systems can be resistant too. So, if you’re working within the eating disorder field, my advice is to take the skills you have gained through ISTDP about working with resistance and use them to help you make the system more open to different ways of working with people.
Moving on to you, what are you struggling to learn right now?
Humility……but that’s my lifelong struggle. In relation to ISTDP, my focus currently is on learning how to teach ISTDP. I’ve been lucky in my ISTDP training to learn from so many skilled and kind people, but I know there are lots of other people I haven’t learned from. So, I’m trying to take what I’ve learned from people like Allan Abbass, Joel Town and Steve Arthey and to apply it in a way that allows me to remain consistent to the model, but flexible enough to still be me and to engage learners in the model.
It’s a complex model and it takes time to learn and I truly think it works best when we’re ourselves because the model is really about connecting. When I started out, I used phrases that came from articles and books, or from watching other people’s tapes. I think this is completely normal, but as I progressed I noticed that I did less of that and that seemed to make a difference. I still used pressure, clarification and challenge, but I was doing it as me. So my struggle is about translating that into my training of others.
Do you have other studies in the pipeline? Will we see an Australian RCT of ISTDP for ED in the future?
Currently I’m taking a break from writing. It’s a labour of love that I currently don’t have the love for. But everyday is a research day in the office. Every day is about gathering the data and analyzing it with my co-researchers (the patients). Although I'm not doing RCT:s at the moment, I still consider myself a researcher and encourage everyone doing this work to adopt a similar approach. Every session is about gathering the data and looking at it and making sense of it and putting it to good use with the patient, whenever I can.
If you dream a bit, where would you like ISTDP and the treatment of eating disorders to go within the next 5 or 10 years?
That’s an easy one to answer… it’s been my dream from the start: To see ISTDP-based residential treatment facilities for eating disorders. I think the model has so much to offer and that it could make such an important contribution to the development of eating disorders treatment. I suspect that offering it in that format would help bring about some great results. My utmost respect goes out to people like Kristy Lamb from BOLD Health who set out down that path for addictions, and so many of the other amazing researchers in ISTDP like Katie Aafjes-Van Doorn at Yeshiva University, Joel Town and Allan Abbass at the Centre of Emotions and Health in Halifax, Canada. We’re so lucky to have those people producing empirical research for the rest of us to have. It’s that kind of leadership that will help us bring more ISTDP therapy into the world.
Want to read more about ISTDP and eating disorders? Make sure you check out this old gem by Dion, Steve Arthey and Allan Abbass on eating disorders and fragility: Intensive Short-Term Dynamic Psychotherapy for Severe Behavioural Disorders: A Focus on Eating Disorders
If you liked this Dion Nowoweiski interview, you might find some of our other interviews interesting. Related to this one, you might be interested in the interviews with Kristy Lamb, Allan Abbass or José Verpoort-Douw. Here's a list of our eight latest interviews:



Diskussion